Ultrasound Case Study
Scaphotrapeziotrapezoid joint osteoarthritis
Stuart Wildman, Extended Scope Physiotherapist/MSK Sonographer
Once you have recovered from the ‘tongue-twister’ of a title…I hope you will find this useful.
The Scaphotrapeziotrapezoid (STT) complex can be overlooked as a source of symptoms within musculoskeletal assessment clinics. It is the second most common cause of wrist arthritis, which often causes surprise.
Patients typically present with a diffuse aching pain in the radial aspect of the wrist, potentially in the distribution. It is often aggravated with gripping,and repetitive upper limb activities.
It is complex to diagnose,partly due to the difficulty differentiating between local common sources of pain such as the Abductor Pollicis Longus/Extensor Pollicis Brevsi/ Flexor Carpi Radialis tendons, De Quervains tenosynovitis, 1st Carpometacarpal joint(1st CMC) and Radiocarpal joint osteoarthritis, bony pathology of the Scaphoid, and potentially trigger thumb. A systematic and structured clinical examination, can differentiate these structures to a point. Plain radiographs can detect and demonstrate STT arthritic change, however many cases of STT are not clinically relevant (Wollstein et al, 2012). The same can be said for other forms of imaging such as MRI.
This patient presented with a 1 year history of an intermittent catching pain over the radial aspect of the wrist. He previously underwent a successful ultrasound guided injection of the STT joint which offered him six months complete relief from his symptoms. Unfortunately, his symptoms returned and he had been re-referred.
During the clinical examination, there was a significant restriction of radial deviation which was uncomfortable. There was no tenderness through the region of APL and EPB, and 1st CMC compression was unremarkable, although there was some joint line tenderness on palpation. Radiocarpal joint flexion and extension were unremarkable. Resisted wrist extension/flexion was unremarkable. It was difficult to localise his symptoms from the clinical examination.
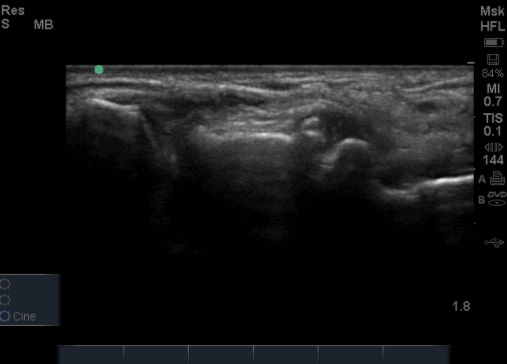
On office based ultrasound a localised effusion and prominent osteophyte was noted over the articulation of the trapezium and scaphoid (Figure 3). As using ultrasound dynamically, I was able to directly use the probe to palpate this joint line which specifically reproduced his pain. This is a useful advantage of using diagnostic ultrasound in clinic when trying to be specific to a patients source of symptoms. There was no visible effusion in the 1st extensor compartment tendon sheaths, and no significant changes of the radiocarpal joint or 1st CMC joint.
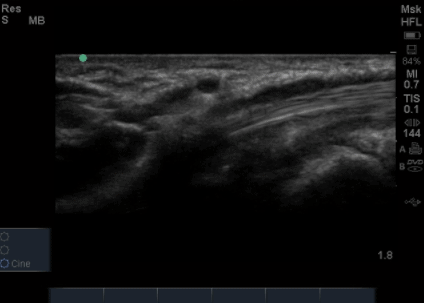
It was also noted that there was an effusion in the tendon sheath of the flexor carpi radialis tendon (Figure 4). This was somewhat unexpected as there was no pain with resisted tests. Interestingly, it has been noted that joint articulations can communicate with the tendon sheaths of both flexor and extensor tendons around the wrist (Boesen et al, 2009). This finding is therefore a potential red herring.
Given the ongoing severity and impact of the pain this patient was experiencing with this case of Scaphotrapeziotrapezoid joint osteoarthritis , they have now been referred for an Orthopaedic opinion. Previous guided injections only offered 6 months relief, and therefore it was not considered appropriate to repeat.
A useful free text article is by Smith et al (2011) which reviews the accuracy of sonographically guided and palpation guided STT injections.
Hopefully you have learnt something from this case study, as always , please share via the links below.

0 Comments