Ultrasound Case Study
Two cases of De Quervain’s Tenosynovitis. TSV or not TSV – that is the question?
Dr Allister Taggart, Consultant Rheumatologist
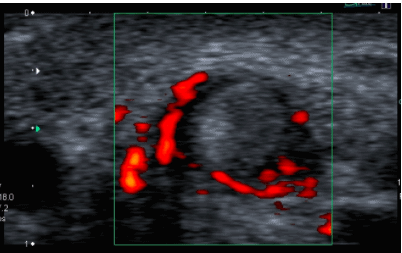
For those sonographers, like myself, who deal with a lot of inflammatory disease, Doppler has become an important part of the sonographic assessment of any patient. Take the tenosynovium as an example. Tenosynovitis (TSV) is best assessed using a transverse probe position so that one gets a view of the whole tendon and its surrounding sheath. Tenosynovitis is often seen as a “ring of fire” around the tendon and this represents increased vascularity of the tenosynovium.
Figure 1 shows the transverse scan of the first dorsal compartment of the wrist in a 33 year old nursing mother who developed classical features of De Quervain’s tenosynovitis just a few weeks after the birth of her baby. The Doppler signal is seen within an expanded hypoechoic tenosynovium but the tendons themselves (abductor pollicis longus and extensor pollicis brevis) are also swollen. These features are best seen where the tendons are closely apposed to the radial styloid by the overlying extensor retinaculum.
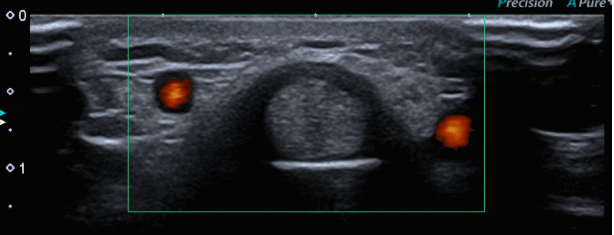
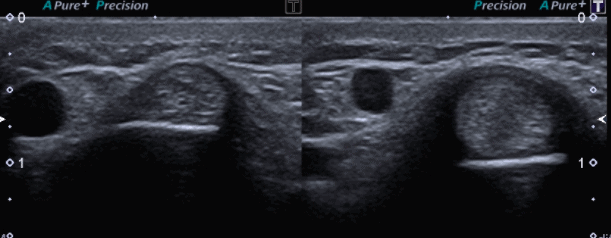
In contrast, Figure 2 shows the transverse scan of the first dorsal compartment of the wrist in a 42 year old male production worker who also complained of classical features of DeQuervain’s tenosynovitis. These had been present for over a year. In this case, the extensor retinaculum appeared thickened and hypoechoic but Doppler scanning revealed no abnormal vascular signal in the tenosynovium. Comparison with the asymptomatic side highlighted the swelling of the inflamed thumb tendons as well as the overlying retinaculum (Figure 3).
Does this mean that the second patient did not have De Quervain’s tenosynovitis? Not at all. Case 1 represents the acute phase of the condition whilst case 2 exemplifies the more chronic stage. In the acute phase, there may be an effusion of the tendon sheath as well as increased vascularity. The effusion will be found distal to extensor retinaculum and beyond the radial styloid.
Recognition of these two stages of the disease may be of practical as well as theoretical importance. The chronic stage is usually less responsive to rest and local corticosteroid injection than the acute stage and may require surgical decompression of the tendons to achieve symptomatic relief(1).
References
1. S. Bianchi, C. Martinoli. Section 10.5.1.1. Pages 449-452. Ultrasound of the Musculoskeletal System. Springer.
0 Comments