Ultrasound Case Study
Deep infrapatellar bursitis
Stuart Wildman, Extended Scope Physiotherapist and MSK Sonographer
This patient presented with chronic left knee pain, which had become recurrently painful over the past year. He noticed some discomfort when swimming and felt a pull in the anterior aspect of the left knee. There was no swelling, bruising or deformity. It has lingered since. He returned to exercise, however, found he has recurrent flare ups of his symptoms which then prevent him from exercising. The knee was particularly sore with activities involving resisted knee extension. He does recall a history of some knee pain, or growing pains, when a child, but can be no more specific regarding a diagnosis. His general health was good.
On examination, there was no effusion or muscle wasting. He had full range of movement of flexion/extension of both knees. There was minimal tenderness on palpation in the patella tendon region of the left knee. Muscle length testing was unremarkable. Ligamentous testing was normal. There was no joint line tenderness.
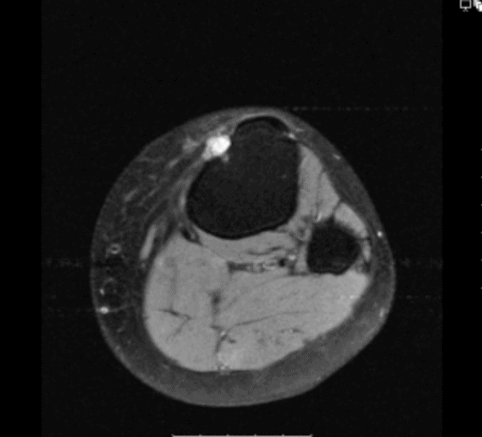
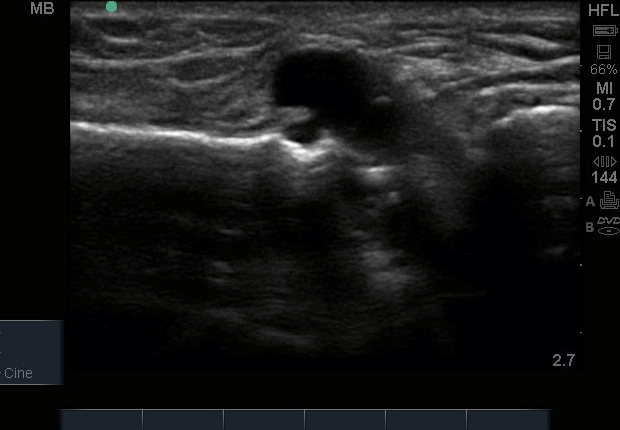
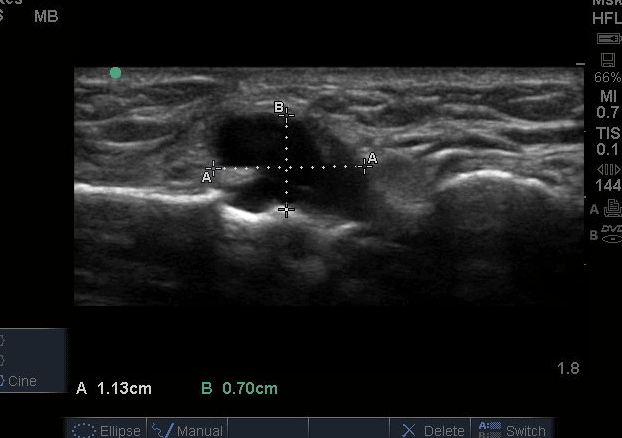
On ultrasound, there was a distended deep infrapatellar bursa, deep to the patella tendon. For those not familiar with this ultrasound image, please see the labelled, to enable yourselves to orientate yourself with the anatomy.
A comparison can be visualised with the asymptomatic knee in the images attached. Patella tendon appeared to be intact with no tendinopathic change. There was a degree of vascularity on the tibial surface , adjacent to the deep infrapatellar bursa.
It is worth noting that you can obtain false negatives if only scanning in the sagittal plane over the patella tendon. Often bursal fluid can pool into either the lateral or medial pouches, forming the characteristic ‘hour glass shape’. This was not evident in this case, but you can see how the bursa was primarily distended towards the medial aspect of the patella tendon in the transverse view.
In summary he appears to present with a chronic deep infrapatella bursitis that is currently flaring up and limiting his activity. This would have been almost impossible to clinically diagnose as it was not possible to reproduce his symptoms on examination. Musculoskeletal ultrasound in clinic has therefore enhanced the assessment this patients has received and enable us to educate him on the specific options of management.


0 Comments