Ultrasound Case Study
Distal patella tendon
Dave Baker, Extended Scope Physiotherapist and MSK Sonographer
This patient presented In their 20's. They reported receiving a kick to the left knee 10+ yrs earlier, there was a significant amount of pain at the time but they never had any formal investigations. Since then they had been aware of a small lump just adjacent to the tibial tuberosity. The patient reported training regularly for the last ten years, and the knee has given few problems. Unfortunately, in recent months they reported noticing pain when load had been placed through the knee. For example when performing yoga and or after heavy periods of training.
The patient had an x-ray which indicated 'a well corticated bony fragment in the patella tendon adjacent to the tibia tuberosity. This may represent either an old ununited avulsion fracture or reminence of Osgood Schlatter's disease. No other significant bony or joint abnormality seen.'
Given the area of her symptoms and the training, they were keen for a further opinion regarding the health of the patella tendon.
On examination, there was point tenderness in the region of the tibial tuberosity. There was full range of movement of the knee, with some discomfort on kneeling and after training.
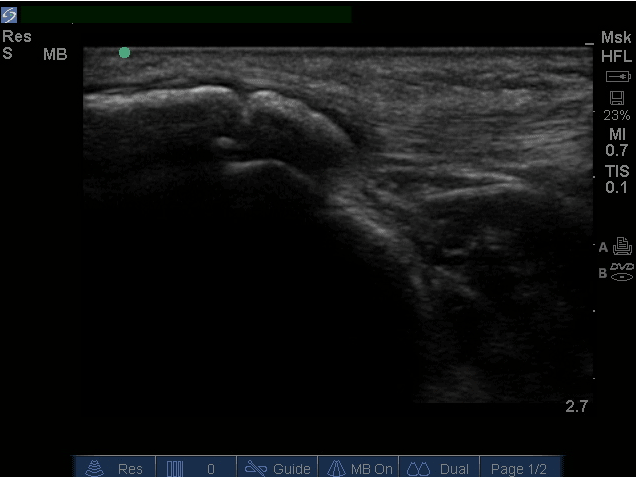
On clinic based ultrasound we were able to visualise a small well corticated, hyperechoic structre that appeared to be a bony fragment, within the distal, medial aspect of the patella tendon lying within the medial fibres measuring 0.5x0.64cm. There was no evidence of any tear in the patella tendon or bursitis. There was a small area of slight thickening of the distal patella tendon fibres just lateral to the hyperechoic fragment. There were no signs of neovascular changes or inflammatory changes on Doppler.
The patients concern was that her knee pain had always been presumed as Osgood Schlatters without any investigation into tendon health. This was something she was keen to establish prior to increasing her training. The use of musculoskeletal ultrasound added to the x-ray, in that we could confirm that the tendon generally looked in good health around the well corticated bony fragment. As mentioned in the x-ray report, the hyperechoic area may have also represented an avulsion fracture given the history of trauma. The patient was ultimately keen to continue to manage this conservatively, and was able to progress with her training with a better understanding of the condition of the patella tendon.
A further reference point is this article by Czyrny (2010) an overview of Osgood Schlatters disease with musculoskeletal ultrasound. Carr et al (2001) also produced a free text article on the patellar tendon and adjacent structures including Sinding-Larsen-Johansson disease and Osgood Schaltters presentations.
 and longitudinal view (right)")

This site is great