Ultrasound Case Study
Loose body of the ankle joint
Stuart Wildman, Extended Scope Physiotherapist and MSK Sonographer
This patient in their 30's attended clinic complaining of several years of difficulties with his right ankle. He was previously a keen snowboarder and reported an initial injury 15 years earlier whilst boarding. He reports a pinching at the front of his ankle whilst boarding, which then limited his ability to dorsiflex his foot and weightbear for a short period. Since this time he has had ongoing flare ups of pain, which have worsened recently as he has started to run for longer periods. He has also noticed intermittent large swellings appearing over the lateral aspect of his ankle, specifically the distal fibula.
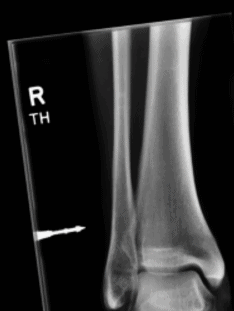
He recalls having an x-ray at the end of last year which was normal. The xray focussed upon the area of soft tissue swelling as you can see by the marker on the AP view. The full report indicates 'No bony abnormality seen. Normal joint spaces. There is minor soft tissue swelling overlying the distal fibula at the site indicated but there is no underlying bony abnormality.' I was able to obtain the images after seeing him in clinic and they are included below, and do show some findings which retrospectively correlate with this patients symptoms.
The ankle did not appear swollen. There was a small soft tissue lump on the lateral aspect of the distal fibula. On examination he presented with some tenderness over the anterior aspect of the talar dome, and also laterally around the peroneals and distal tibfib joint. Dorsiflexion was restricted to 3/4 the normal range and felt tight with some slight discomfort on lunging as well. Plantarflexion, inversion, eversion were preserved. Resisted tests were unremarkable. External rotation test for syndesmosis involvement was negative, as were direct palpation of the distal tibfib joint and compression test.

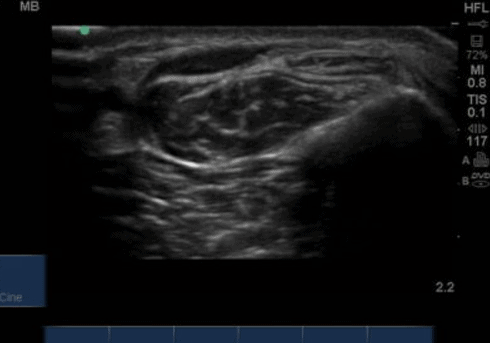



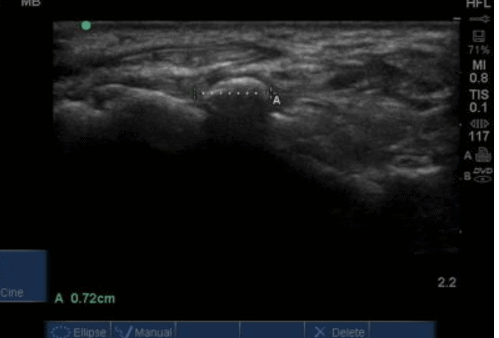
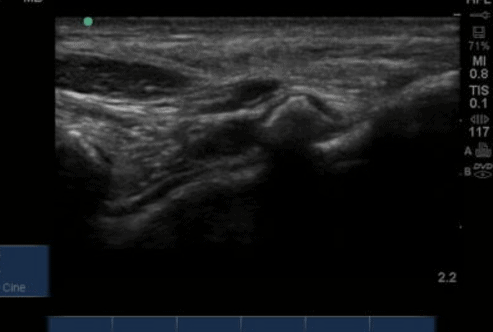
On office based ultrasound peroneus longus and brevis appeared normal and intact. There was an anaechoic fluid collection superficial to them (Figure 3 and 4) and this correlated with the area of swelling he reported. This also tracked slightly medial to the fibula (Figure 5), directly superficial to the distal tibfib joint and potentially communicated with it, although I could not see this clearly. There was no vascularity on doppler, and the anaechoic collection was not compressible. Suggestive of a ganglion, which correlated with the position of my initial observation findings. The ATFL and CFL ligaments were also intact on the lateral aspect of the ankle. I then turned my attention to the anterior aspect of the talocrural joint, as this correlated clinically with the mechanism of his injury and also the ongoing aggravation he was experiencing with dorsiflexion. Palpation of the anterior talus in a position of plantarflexion was uncomfortable.
On visualising the anterior talocrural recess, I became aware of a large hyperechoic lesion in the recess itself (Figure 6), both in long and short axis views. On dynamic testing this appeared to move seperately to the talus during dorsiflexion, which you can see in the video below.
This appears to present as a loose body of the talocrural joint, and shows the benefit of using MSK ultrasound dynamically to integrate tissues. It also demonstrates the added benefit of ultrasound over other forms of imaging although some small potential loose bodies can be seen on the lateral x-ray. This patient has now been referred for an MRI and will potentially have Orthopaedic input. I will update the case with MRI images when available.
0 Comments