Ankle and foot ultrasound
What structures can we see at the ankle and foot?
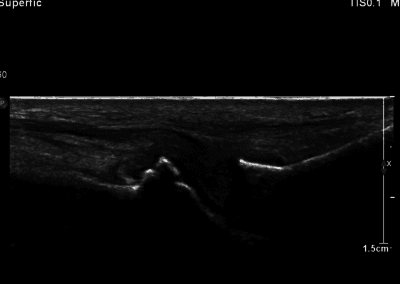
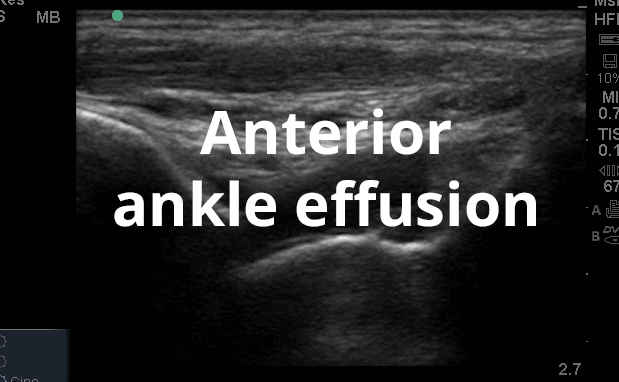
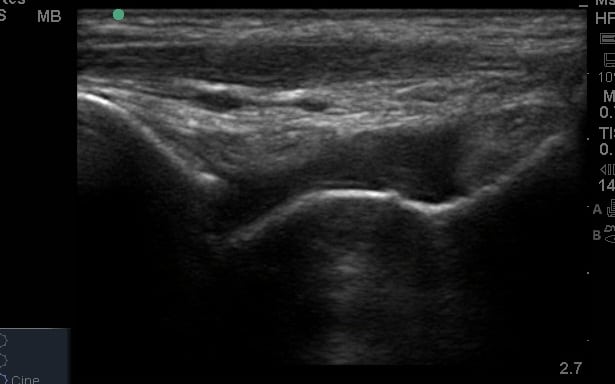
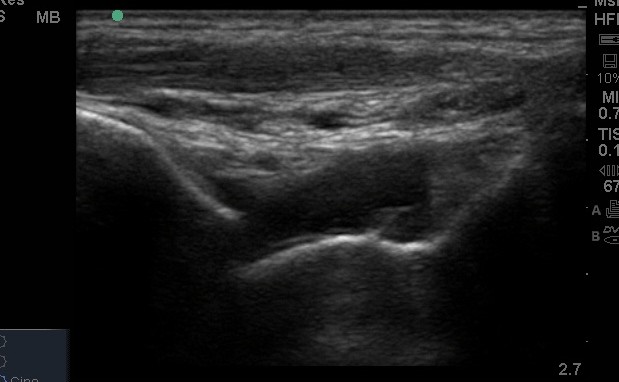
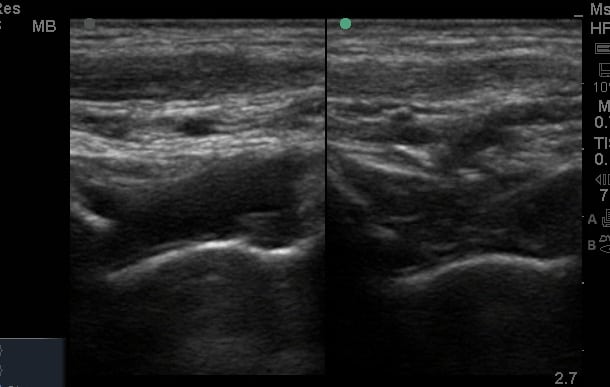
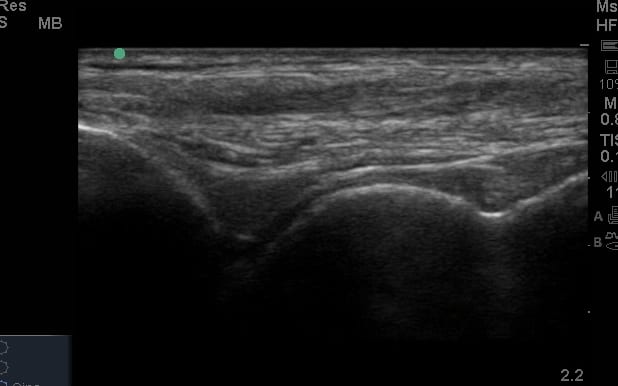
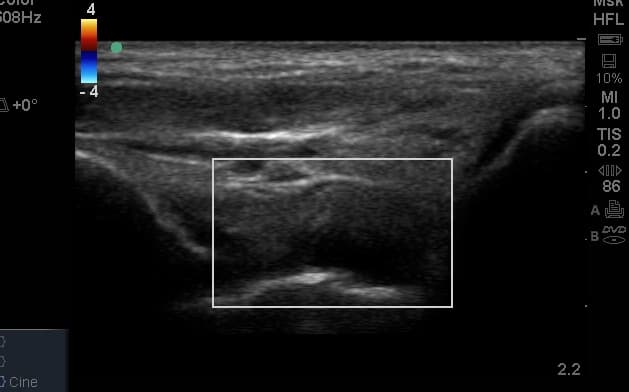
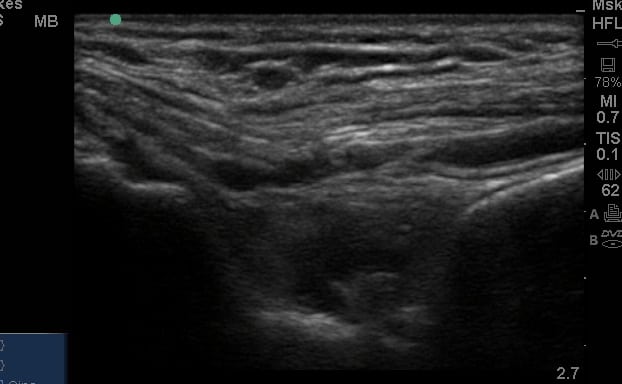
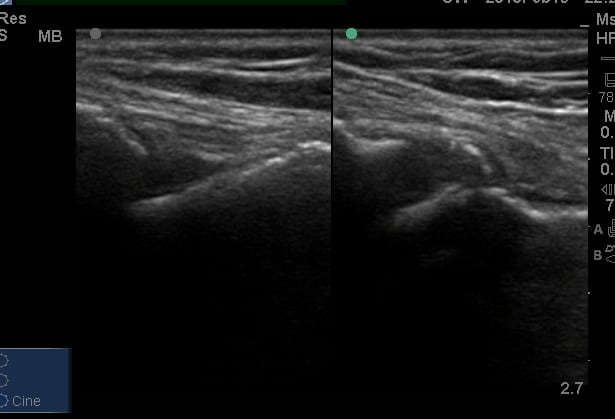
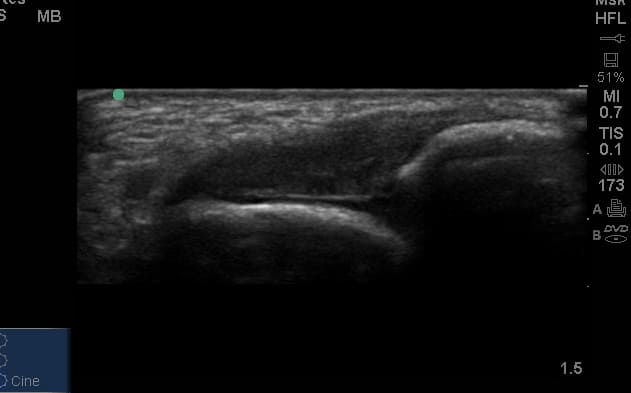
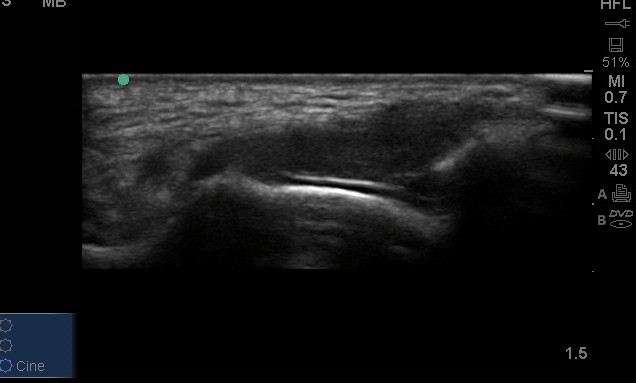
Many of the clinically important structures around the foot and ankle can be seen clearly on diagnostic ultrasound. The stabilising ligaments of the lateral aspect of the ankle, for example, as well as the tendons which travel from the lower leg to the foot, can all be scanned in their entirety to see for pathology, localised effusion. Ultrasound scan evaluation of the anterior aspect of the ankle joint can also identify pathology, such as osteoarthritic changes and joint effusions. Structures that can be clearly visualise include:
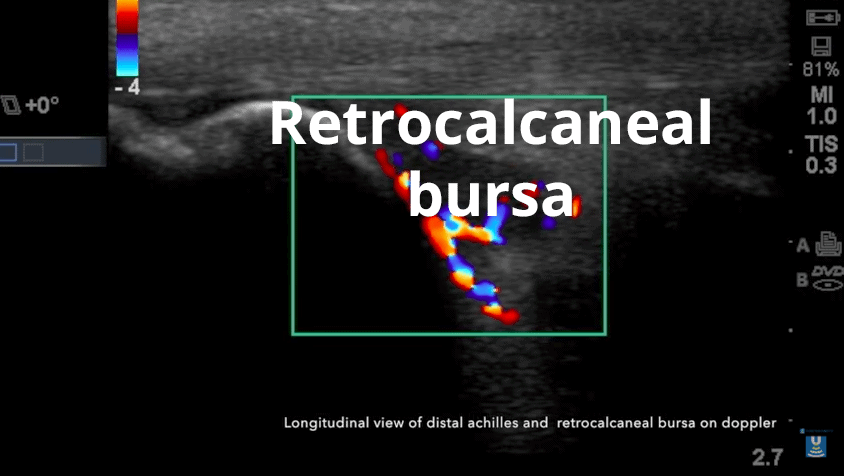
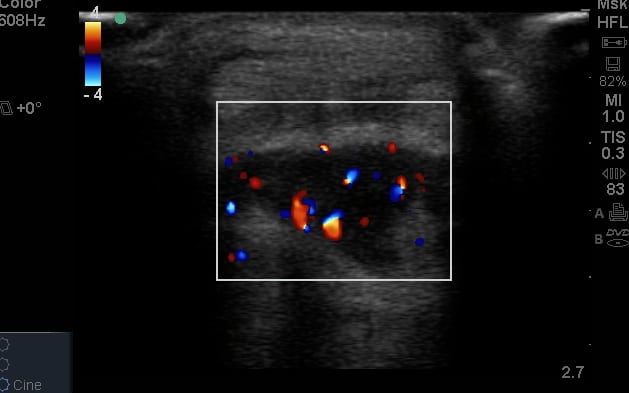
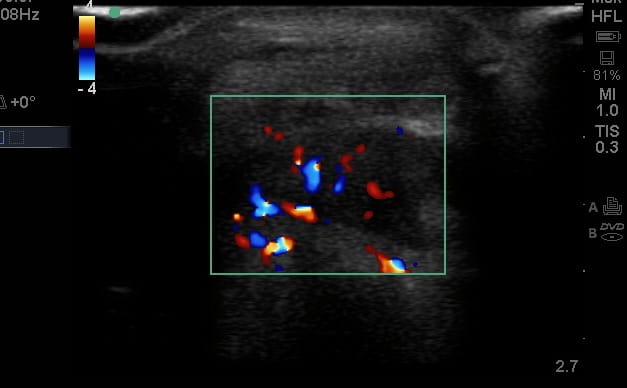
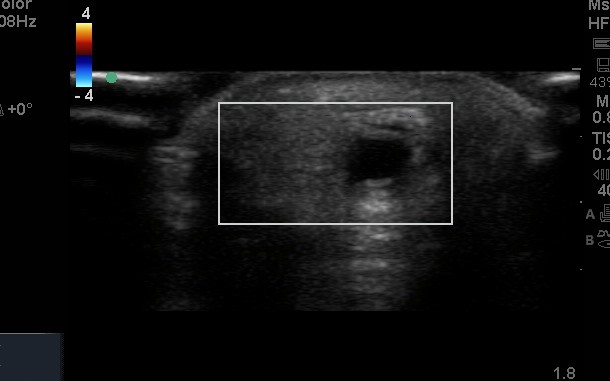
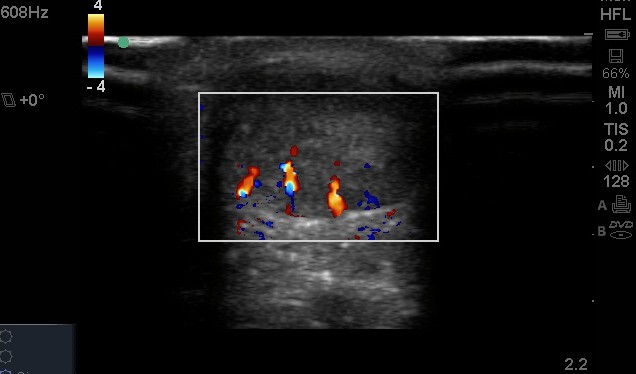
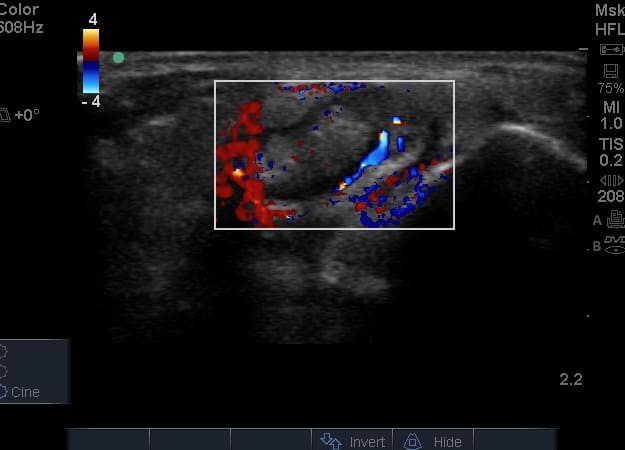
- All joint articulations including the talocrural, talnonavicular, calcaneocuboid, naviculocuneiform, subtalar, midtarsal and metatarsophalangeal joints. With the use of doppler, hyperaemia can be assessed and synovitis detected.
- Neurovascular structures can be easily visualised including the dorsalis pedis, tibial nerve, peroneal nerves
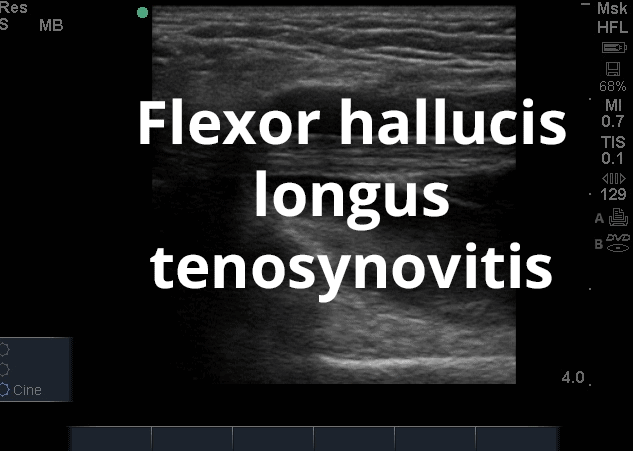
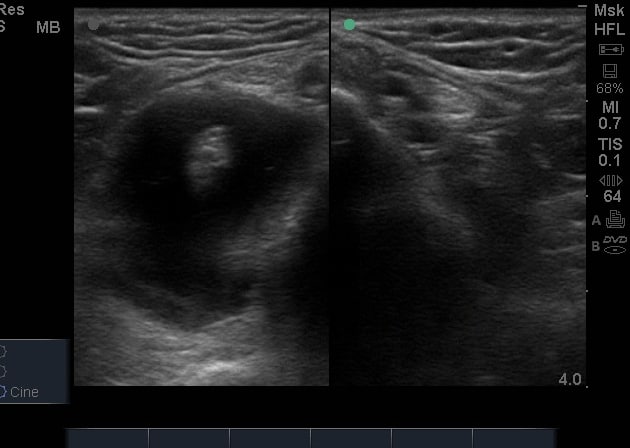
- Medial soft tissue structures such as the tibialis posterior tendon, flexor digitorum and flexor hallucis.
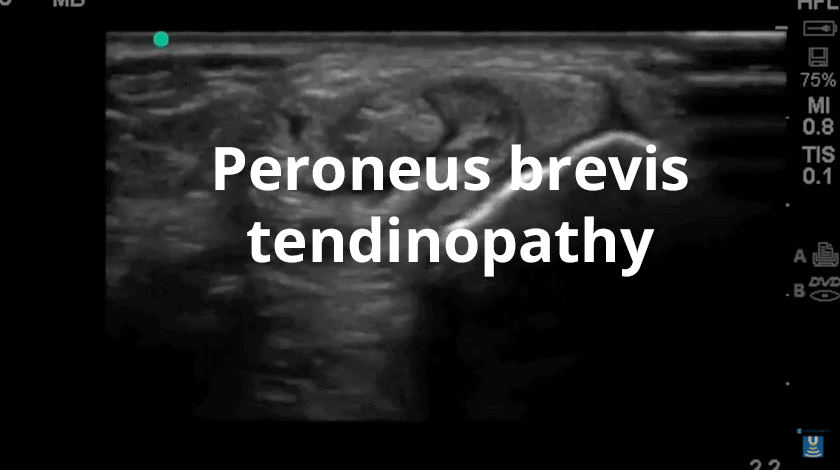
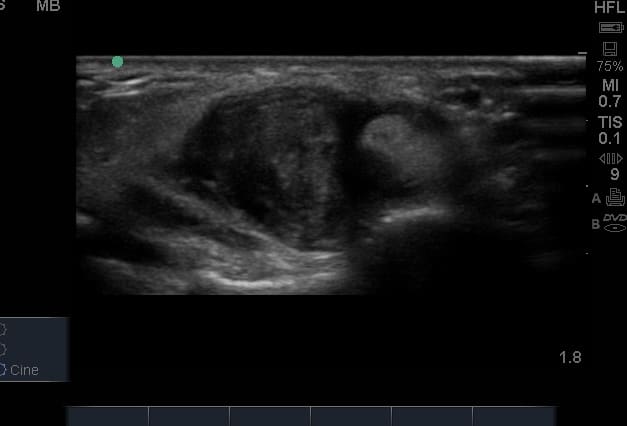
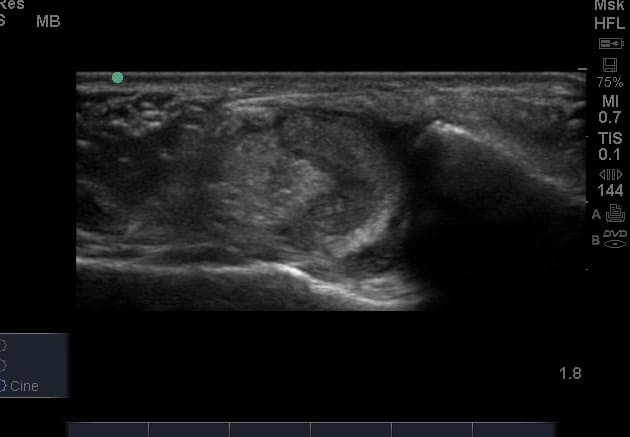
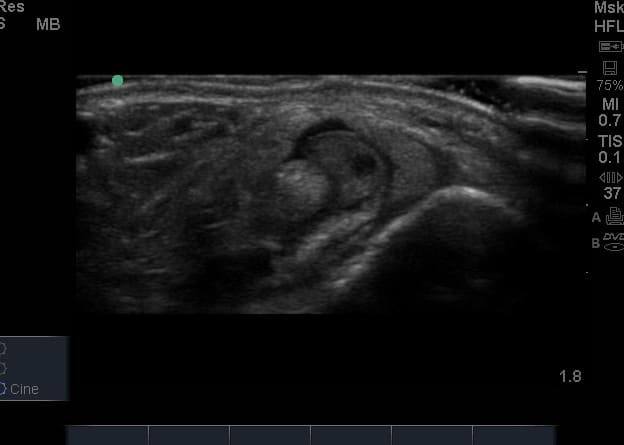
- Lateral soft tissue structures including peroneus brevis and longus inc. dynamic interrogation.
- Ligamentous structures surrounding the ankle joint including the Anteriortalofibular ligament, Calcaneofibular ligament and the Syndesmotic region.
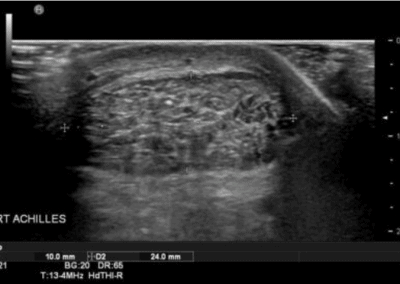
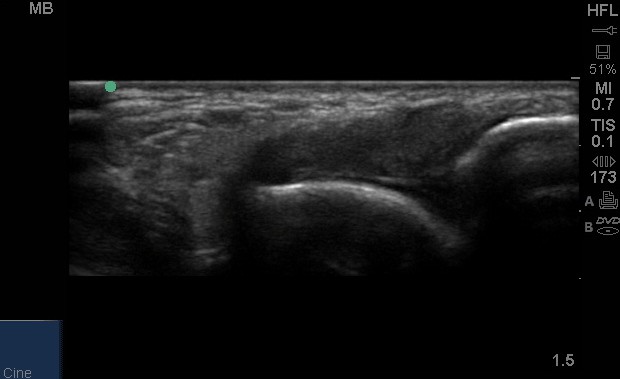
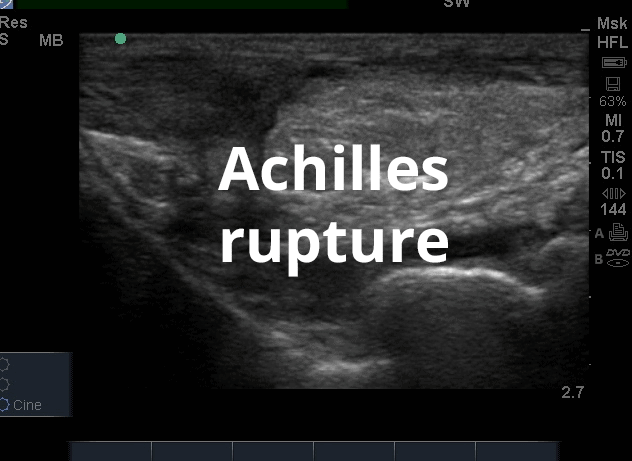
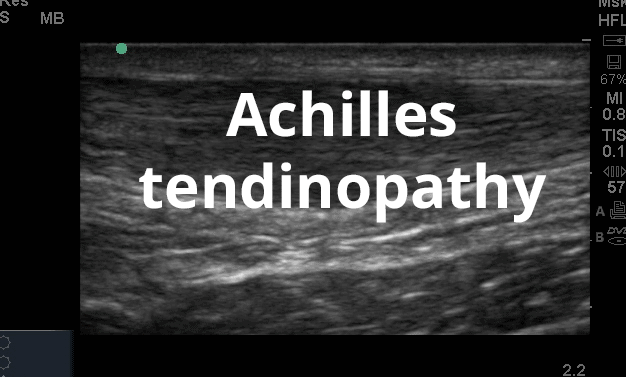
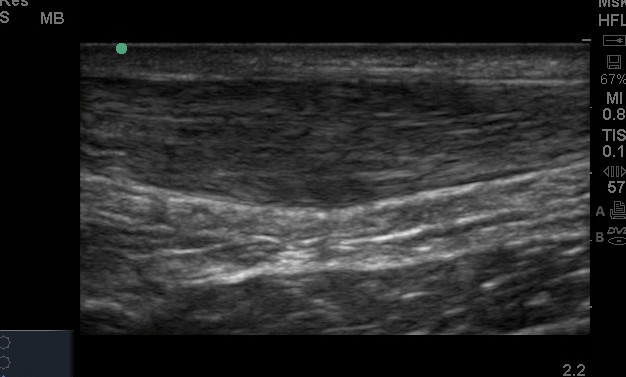
- Posteriorly, the achilles tendon and associated structures are well visualised.
- Superficial cortex of bony structures to assess for fractures and bony pathology.























Videos
Register to receive our newsletter including case studies
Anatomy
The ankle and foot region has complex anatomy. This is well beyond a brief paragraph here! So we will attempt to summarise the key anatomical structures. The ankle is composed of three articulations - the distal tibiofibular joint (syndesmosis), the ankle joint itself (the talocrural joint) and the subtalar joint (talocalcaneal). The talocrural joint is stabilised by medial and lateral ankle ligaments, with the lateral ligament complex being more commonly injured and visualised under ultrasound. Commonly, the medial and lateral tendons are the symptomatic regions that are investigated by ultrasound and clinical examination. These are listed in the introduction to this page. Neurovascular structures include anteriorly the deep peroneal nerve and anterior tibial artery, laterally the superficial peroneal nerve and medially the tibial nerve and posterior tibial artery.
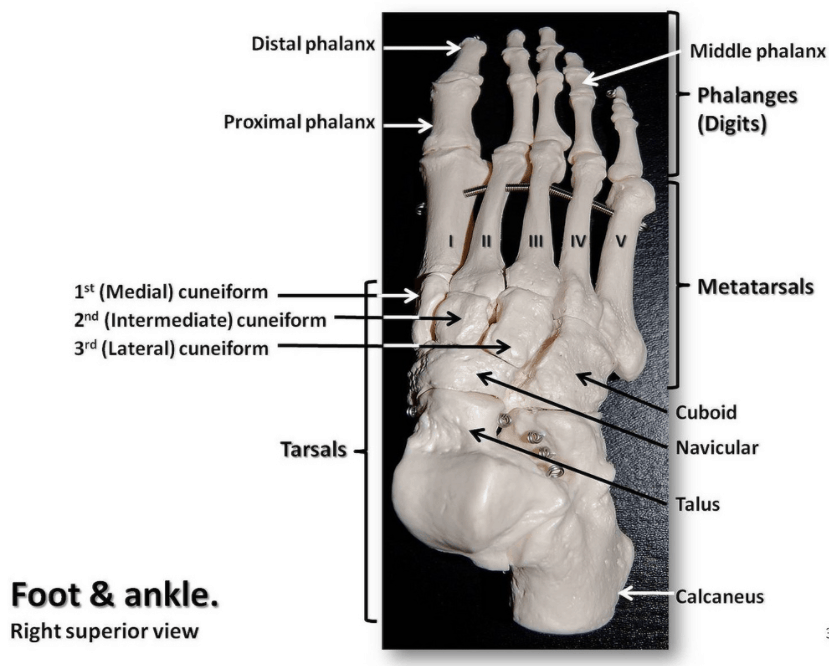
Moving into the foot, the anatomy is arguably more complex with 28 bones, 30 joints and more than 100 muscles ,tendons and ligaments. Ensuring you have a comprehensive 'blue print' of the bony anatomy is important when using ultrasound in this region, and layering the soft tissue structures onto this.