Knee ultrasound
What structures can we see at the knee?
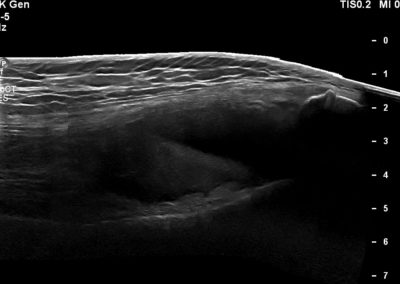
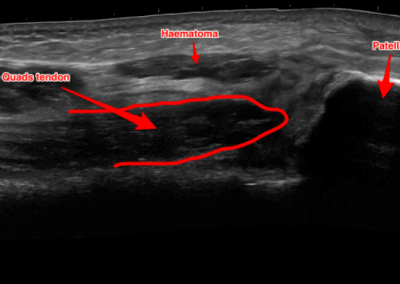
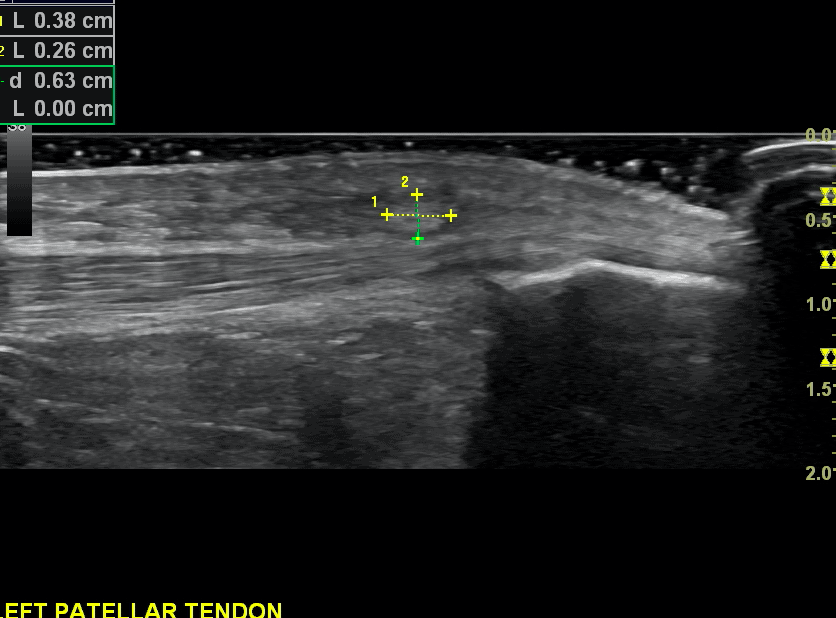
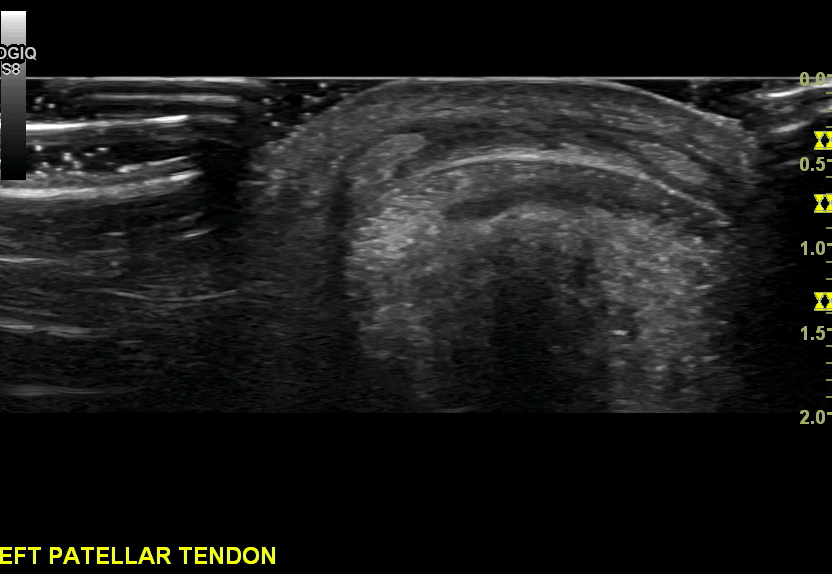
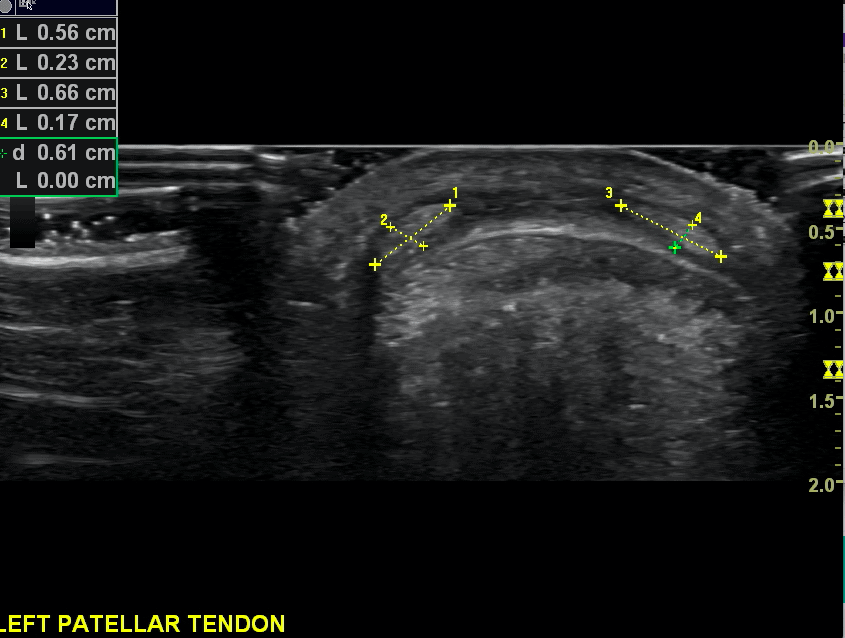
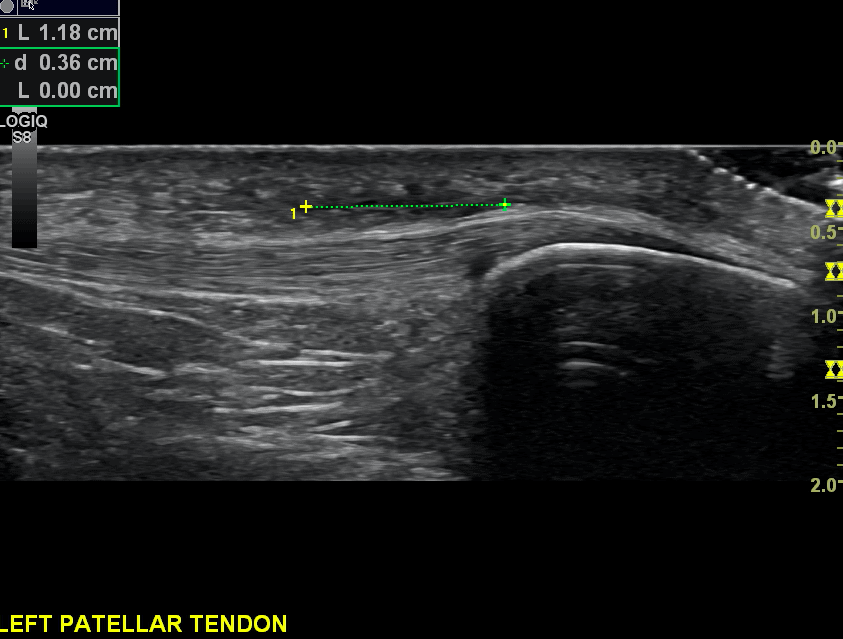
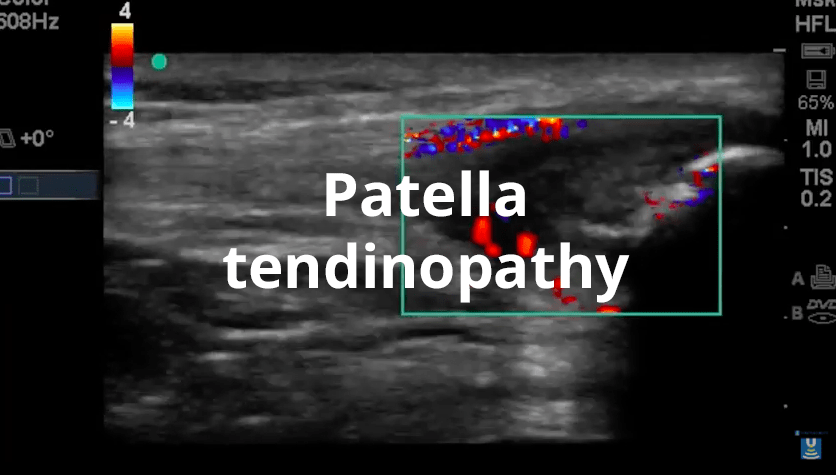
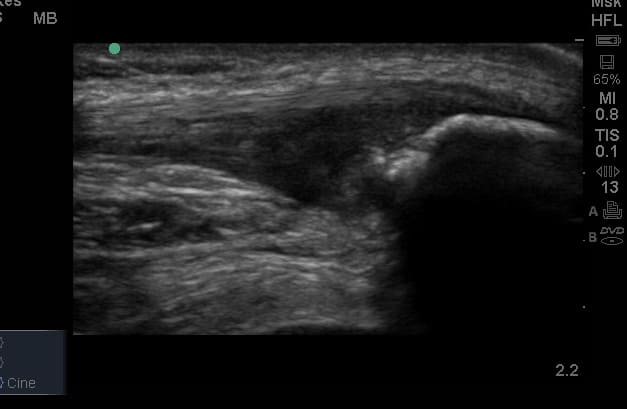
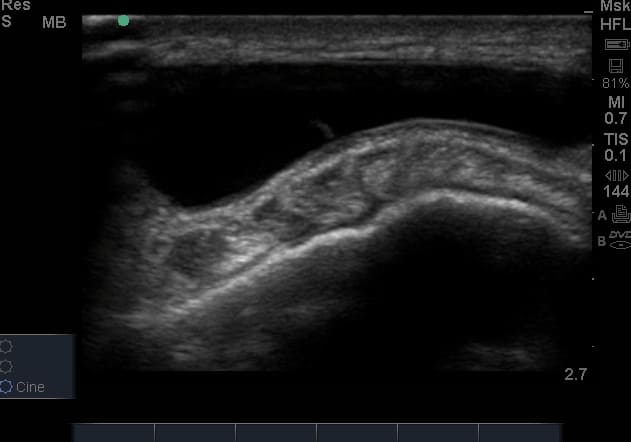
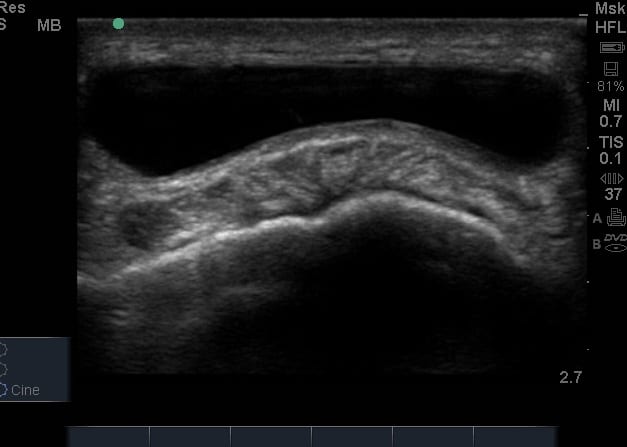
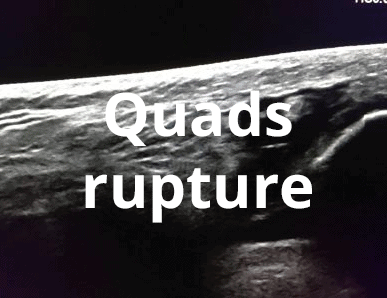
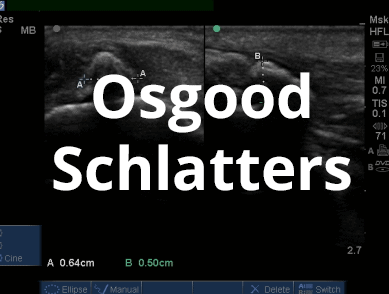
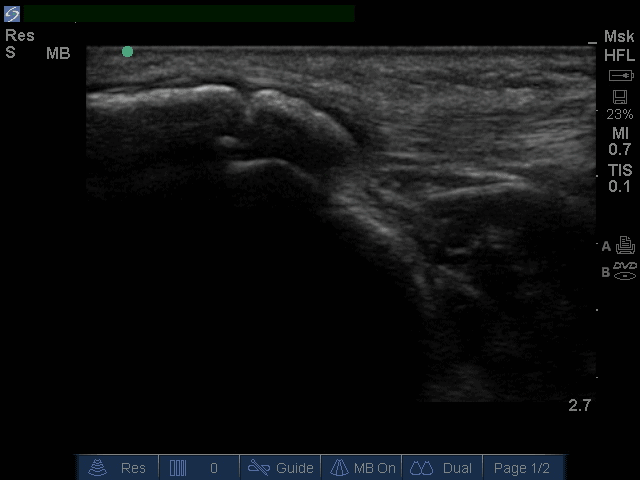
- Patella and quadriceps tendons
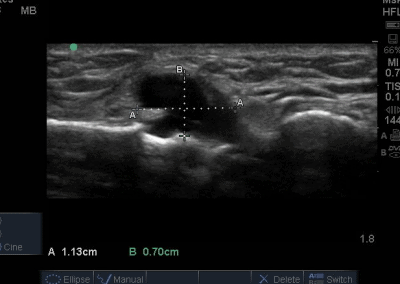
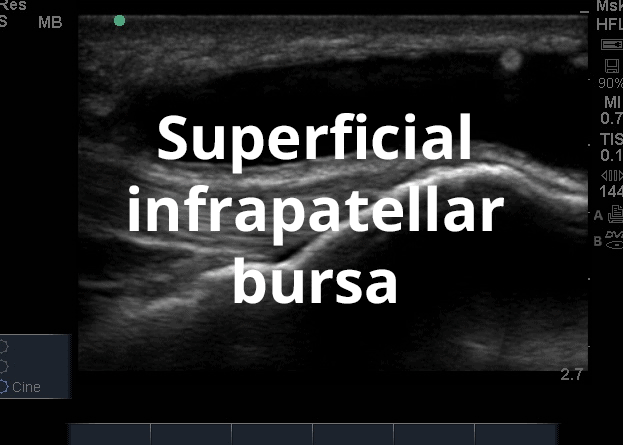
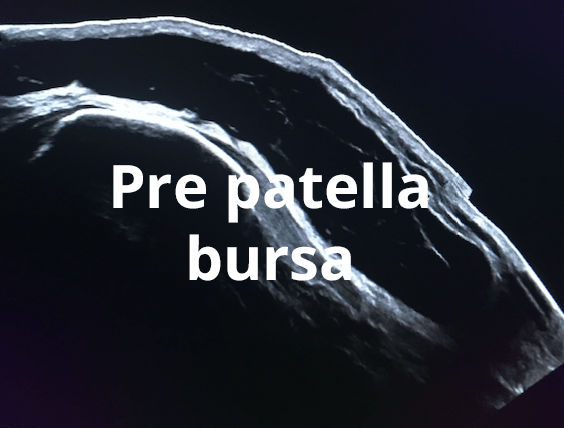
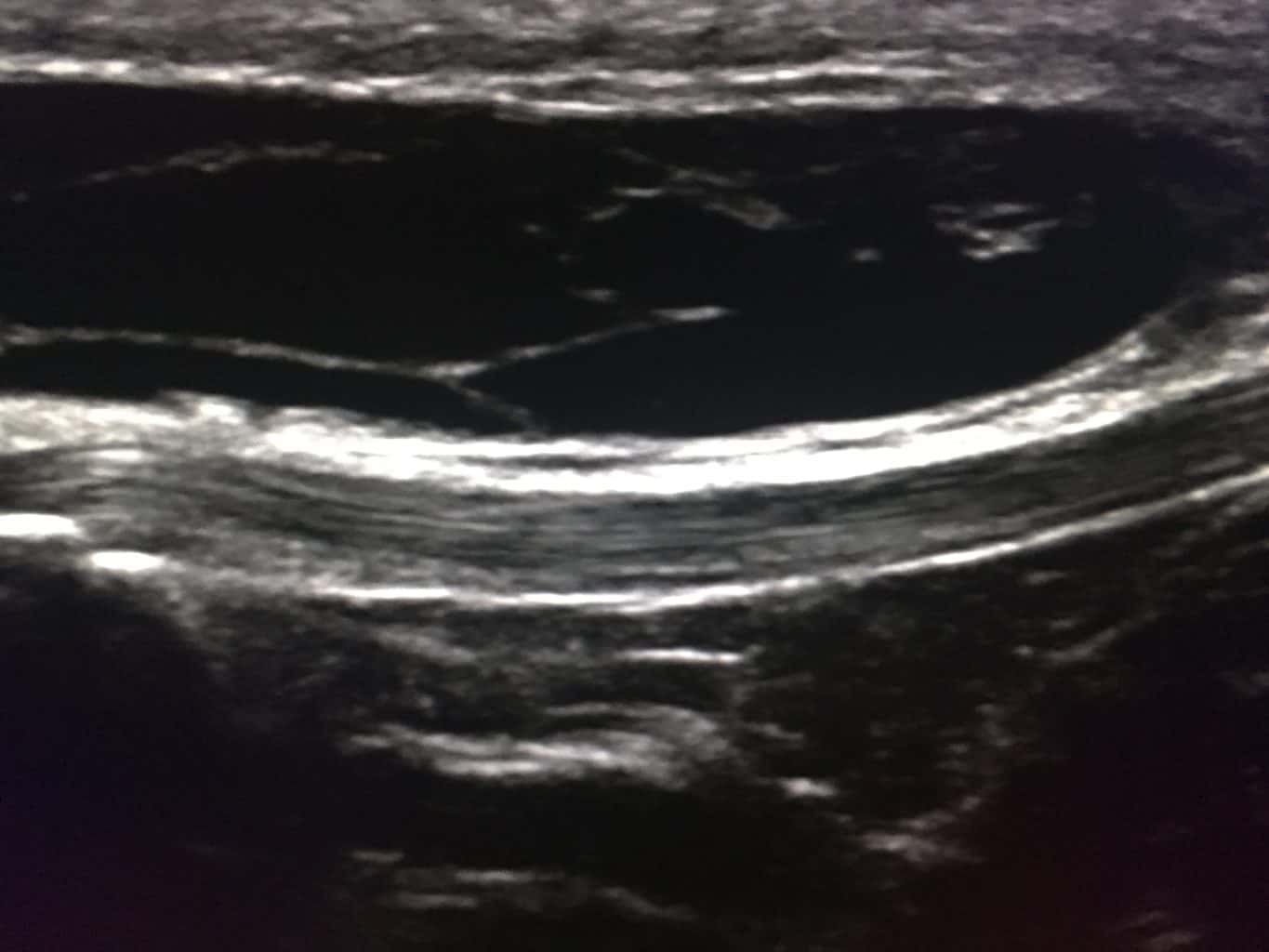
- Several knee bursae
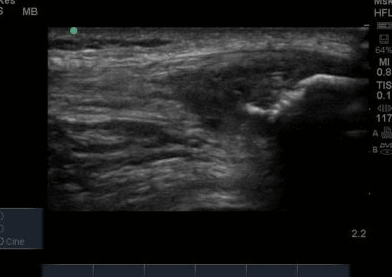
- Muscle and tendinous structures anterior and posterior to the joint
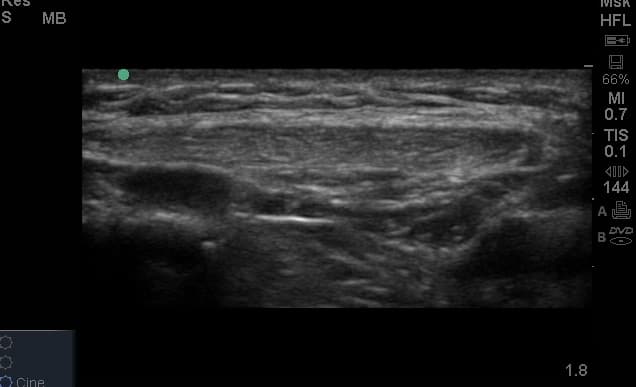
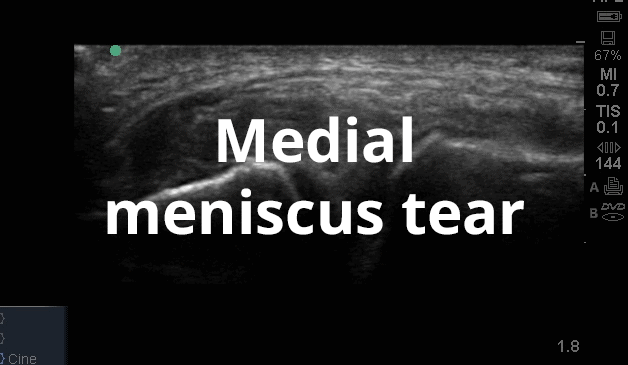
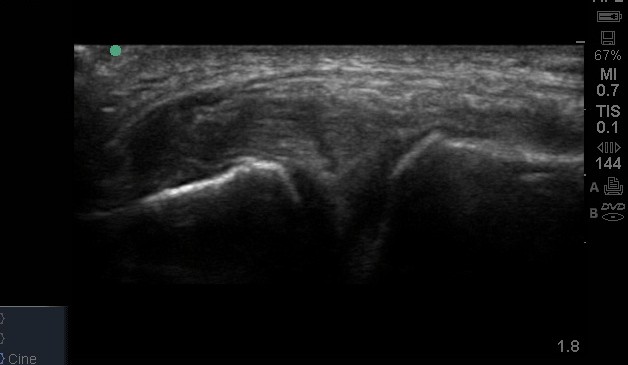
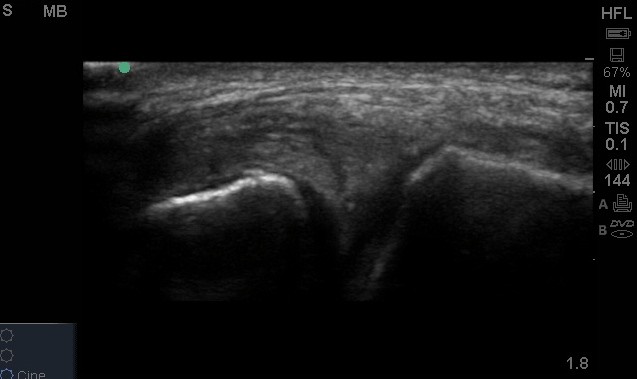
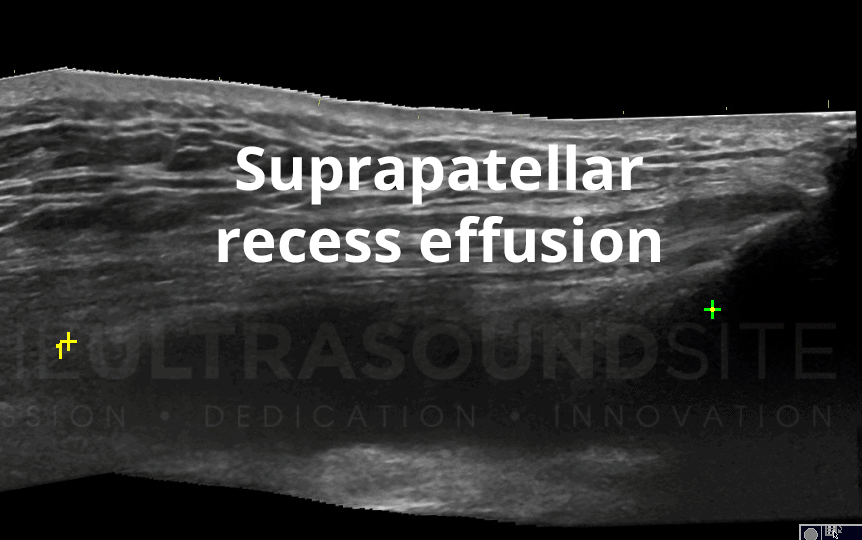
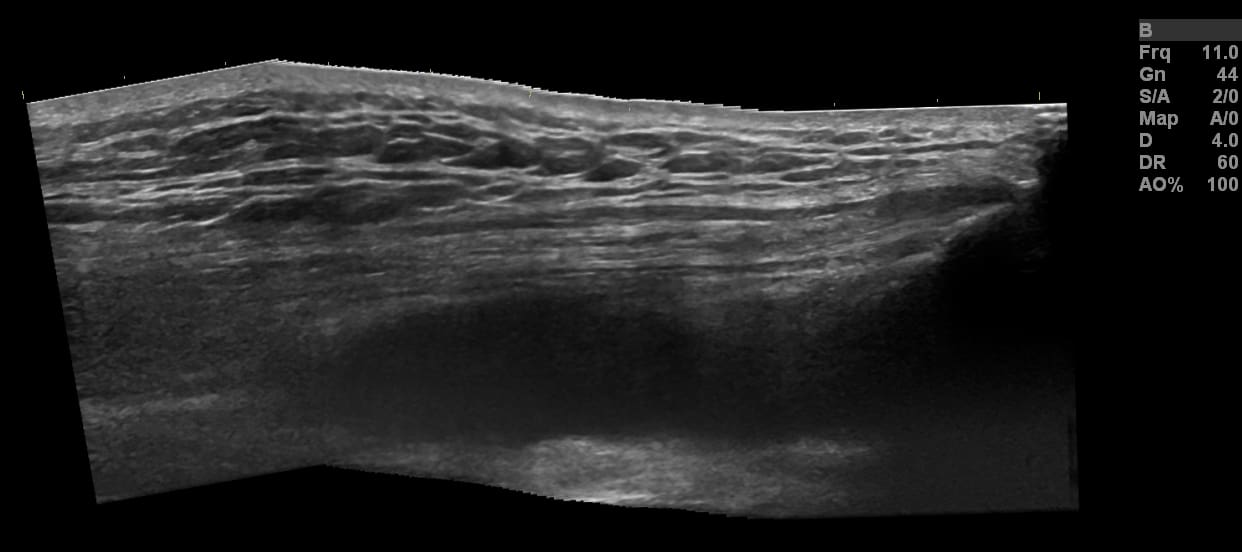
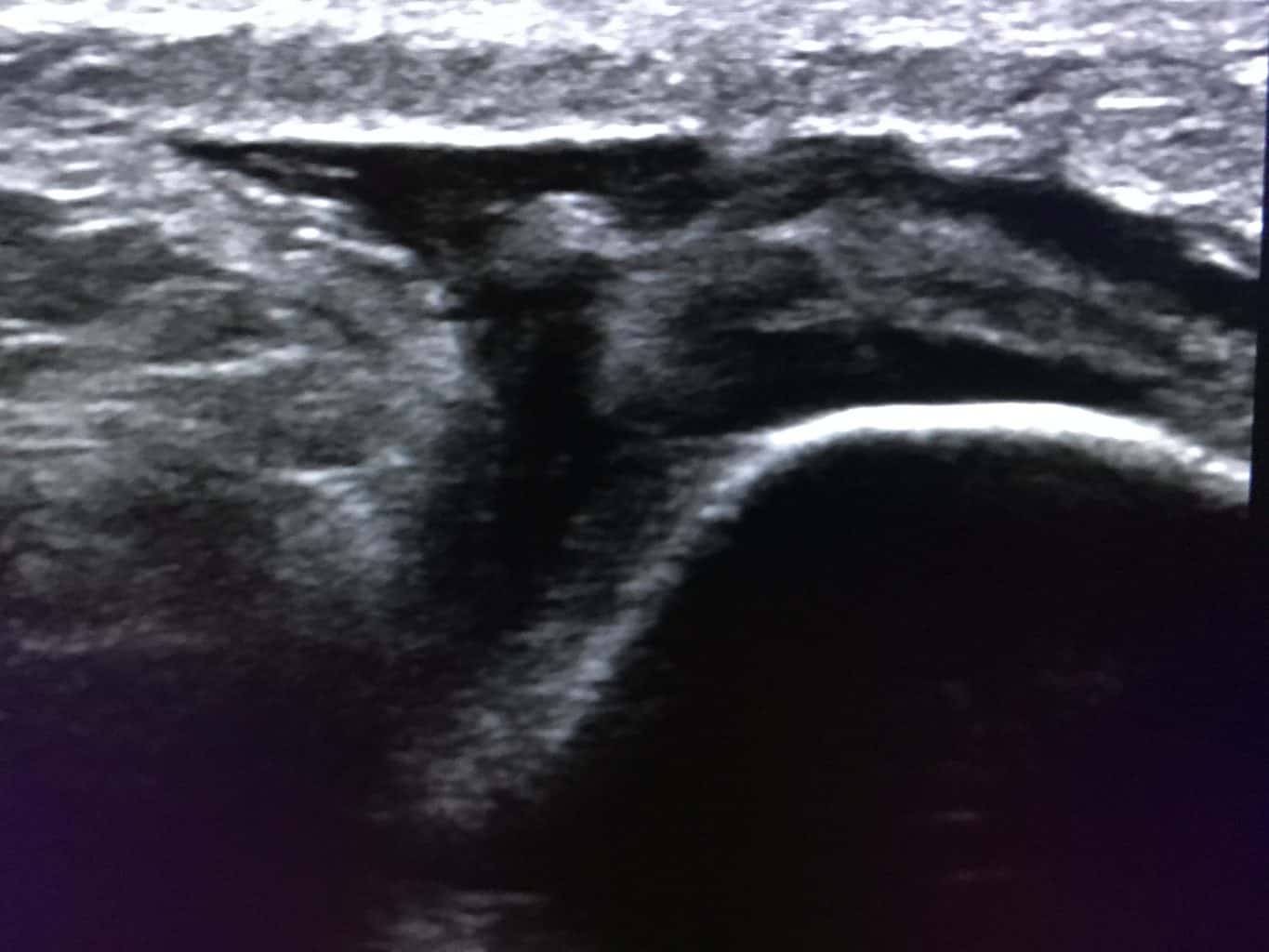
- Joint lines and capsular recesses

Case Studies
We have put together a series of case studies which describe how ultrasound was utilised alongside a clinical examination. Discussing how its use did or did not change the patient journey, alongside some useful references.
Gallery























Join The Ultrasound Site on MedShr to discover and discuss fascinating cases
Ultrasound Pathology Videos
Register to receive our newsletter including case studies
Anatomy
There are numerous important soft tissue structures surrounding the knee joint. Anteriorly, the extensor mechanism consists of the quadriceps muscle, the quadriceps tendon and the patella tendon distal the patella tendon which inserts onto the tibial tuberosity. Posteriorly tendons can be viewed as medial and lateral groupings. This also assist with how to approach them from an ultrasound perspective. Laterally, the biceps femoris distal tendon, which emerges from the short and long heads of the muscle is most prominent. Also , the lateral head of the gastrocnemius muscle and the popliteus. More distally the peroneal muscles originate from the fibular head. Medially, the hamstring tendons of the semimembranosus and semitendinosus muscles travel on the medial aspect of the medial head of gastrocnemius, the classic location for a Bakers cyst. The gracilis and sartorius lie in a more medial postion, ultimately joining the semitendinosus to form the pes anserine complex or the goos foot tendon.
There are several bursae surrounding the knee, highlighted nicely in a freely accessible article by Chatra (2012).
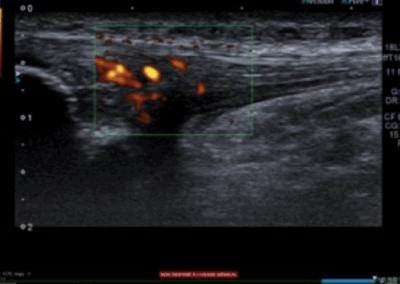
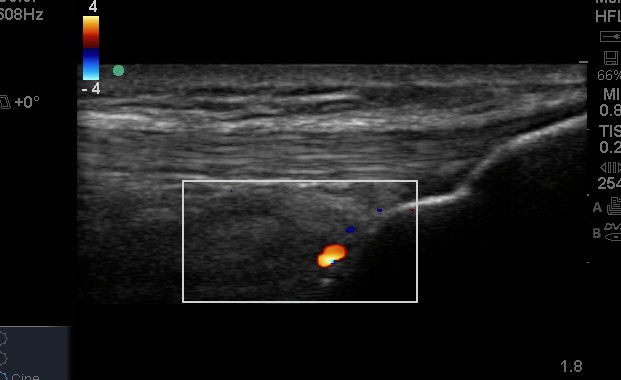
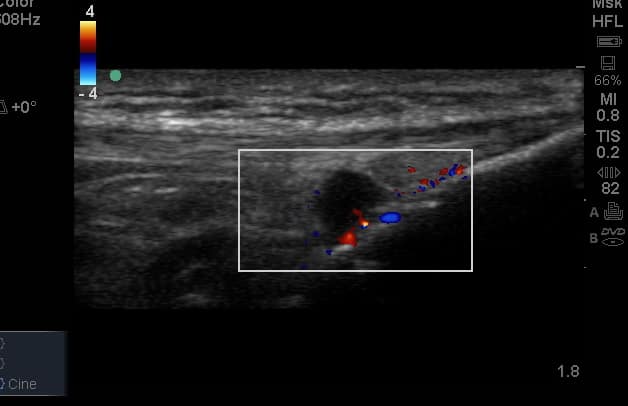
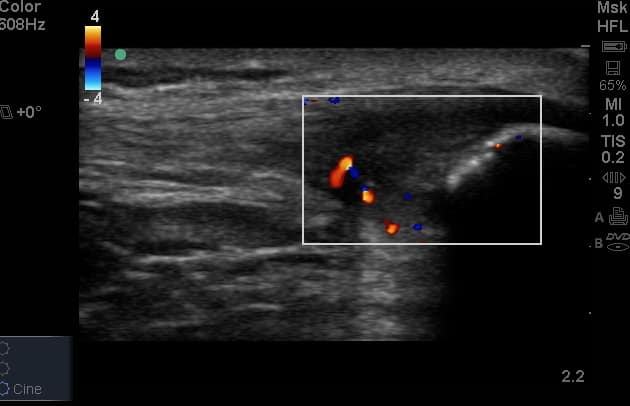
The popliteal fossa is situated posteriorly, formed by the semimembranosus and semitendinosus medially, the bciceps femoris laterally and distally the two heads of the gastrconemius muscle.It contains the popliteal artery, and its geniculate branches to the knee joint and capsule. The popliteal vein is also situiated close to and superficial to the artery. the sciatic nerve descend proximal to the popliteal fossa and divides into the tibial and common peroneal nerves at the apex of the fossa.